








Global

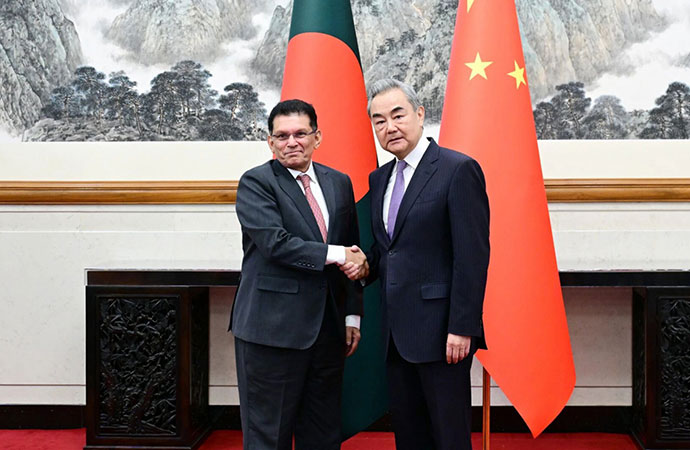
Young passengers wear masks on a high-speed train in Hong Kong, Wednesday, Jan. 22, 2020. At that time, it was hard to know how dangerous the virus would be. (AP Photo/Kin Cheung) AP Photo/Kin Cheung
The Harvard historian Jill Lepore recounted recently in The New Yorker magazine that when democracies sink into crisis, the question "where are we going?" leaps to everyone's mind, as if we were waiting for a weather forecast to tell us how healthy our democracy was going to be tomorrow. Quoting Italian philosopher Benedetto Croce, Lepore writes that "political problems are not external forces beyond our control; they are forces within our control. We need solely to make up our own minds and to act."
And so it is with the coronavirus epidemic. How big will this epidemic be? How many people will it infect? How many Americans will die? The answers to these questions are not written in stone. They are partially within our control, assuming we are willing to take the responsibility to act with commitment, urgency and solidarity.
I am an epidemiologist with eight years of field experience, including time on the front lines of the isolation and quarantine efforts during the 2009 swine flu pandemic. One month ago, I was under the impression that the death reports due to COVID-19 circulation in China were giving us an unfair picture of its mortality rate. I wrote a piece saying that the death rate of an emerging disease always looks bad in the early stages of an outbreak, but is likely to drop once better data become available. After waiting for eight weeks, I am now worried that these new data - data indicating that the virus has a low fatality rate - may not arrive.
Case fatality rate and infection fatality rate By Jan. 31 2020, China had reported a total of 11,821 cases of COVID-19 and 259 deaths; that's about a 2% case fatality rate. Two weeks later, the tally had risen to more than 50,000 cases and 1,524 deaths, corresponding to about 3% case fatality (the rise in the case fatality is expected as deaths always get counted later than cases). For an easily transmissible disease, a 2% or 3% fatality rate is extremely dangerous.
However, case fatality rates are computed using the officially reported numbers of 11,821 cases or 50,000 cases, which only include individuals who (a) experience symptoms; (b) decide that their symptoms are bad enough to merit a hospital visit; and (c) choose a hospital or clinic that is able to test and report cases of coronavirus.
Surely, there must have been hundreds of thousands cases, maybe a million cases, that had simply gone uncounted.
First, some definitions from Steven Riley at Imperial College. The infection fatality rate (IFR) gives the probability of dying for an infected person. The case fatality rate (CFR) gives the probability of dying for an infected person who is sick enough to report to a hospital or clinic. CFR is larger than IFR, because individuals who report to hospitals are typically more severely ill.
If China's mid-February statistic of 1,524 deaths had occurred from 1 million infections of COVID-19 (counting all symptomatic and asymptomatic infections), this would mean that the virus had an infection fatality rate of 0.15%, about three times higher than seasonal influenza virus; this is a concern but not a crisis.
The IFR is much more difficult to estimate than the CFR. The reason is that it is hard to count people who are mildly ill or who show no symptoms at all. If you are able to count and test everybody - for example, on a cruise ship, or in a small community - then you may be able to paint a picture of what fraction of infections are asymptomatic, mild, symptomatic and severe.
Scientists working at the London School of Hygiene and Tropical Medicine, Imperial College London and the Institute for Disease Modeling have used these approaches to estimate the infection fatality rate. Currently, these estimates range from 0.5% to 0.94% indicating that COVID-19 is about 10 to 20 times as deadly as seasonal influenza. Evidence coming in from genomics and large-scale testing of fevers is consistent with these conclusions. The only potentially good news is that the epidemic in Korea may ultimately show a lower CFR than the epidemic in China.
Impact of the epidemic in the US
Now that new COVID-19 cases are being detected in the U.S. every day, it is too late to stop the initial wave of infections. The epidemic is likely to spread across the U.S. The virus appears to be about as contagious as influenza. But this comparison is difficult to make since we have no immunity to the new coronavirus.
On balance, it is reasonable to guess that COVID-19 will infect as many Americans over the next year as influenza does in a typical winter - somewhere between 25 million and 115 million. Maybe a bit more if the virus turns out to be more contagious than we thought. Maybe a bit less if we put restrictions in place that minimize our travel and our social and professional contacts.
The bad news is, of course, that these infection numbers translate to 350,000 to 660,000 people dying in the U.S., with an uncertainty range that goes from 50,000 deaths to 5 million deaths. The good news is that this is not a weather forecast. The size of the epidemic, i.e., the total number of infections, is something we can reduce if we decrease our contact patterns and improve our hygiene. If the total number of infections decreases, the total number of deaths will also decrease.
What science cannot tell us right now is exactly which measures will be most effective at slowing down the epidemic and reducing its impact. If I stop shaking hands, will that cut my probability of infection by a half? A third? Nobody knows. If I work from home two days a week, will this reduce my probability of infection by 40%? Maybe. But we don't even know the answer to that.
What we should prepare for now is reducing our exposures - i.e., our chances of coming into contact with infected people or infected surfaces - any way that we can. For some people this will mean staying home more. For others it will mean adopting more stringent hygiene practices. An extreme version of this exposure reduction - including mandatory quarantine, rapid diagnosis and isolation, and closing of workplaces and schools - seems to have worked in Hubei province in China, where the epidemic spread appears to have slowed down.
For now, Americans need to prepare themselves that the next 12 months are going to look very different. Vacations may have to be canceled. Social interactions will look different. And risk management is something we're going to have to think about every morning when we wake up. The coronavirus epidemic is not going to extinguish itself. It is not in another country. It is not just the cold and flu. And it is not going away.
[You're smart and curious about the world. So are The Conversation's authors and editors. You can read us daily by subscribing to our newsletter.]
Maciej F. Boni, Associate Professor of Biology, Pennsylvania State University
From www.theconversation.com










Leave a Comment
Recent Posts
An onus on skilled economic ma ...
We have now commenced the first full fiscal under the BNP government e ...
How a push to disarm Hezbollah ...
A deal between Lebanon and Israel was billed as paving the way for pea ...
10th Anniversary of the 15 July Coup Attempt: Victor ..
The US military attacked Iran early Wednesday (Jul. ..
The government appointed internationally renowned hu ..
Govt plans sweeping health sector reforms to take sp ..